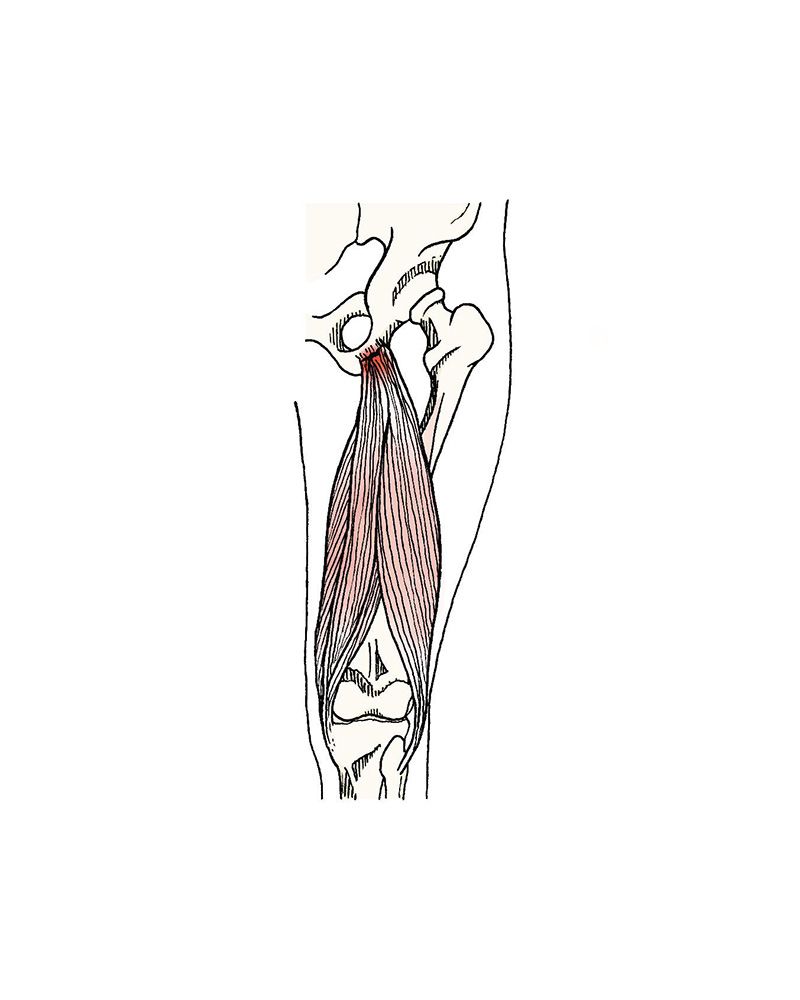
The posterior thigh muscles include the biceps cruralis, the semitendinosus and semimembranosus. Their primary function is knee flexion, and they are also secondary extensors of the hip. These muscles attach to the ischium, the lowest and most posterior bony eminence of the pelvis. In the sitting position, body weight is supported by the ischions. Adjacent to these structures runs the sciatic nerve. It is therefore understood that in cases of pathology tendon tests, irritation of the sciatic nerve can occur.
Ischiotibial and Crural Biceps Tendinopathy
Tendonitis, degenerative tendinosis and myotendinous rupture
The injury can occur acutely, with rupture at the myotendinous junction. Less frequently, the tendon ruptures or pulls out a bony portion at the ischion. The typical mechanism of injury is eccentric contraction of the muscle chains, in the position where the tendons are most stretched, as in a water skier, with flexion of the hip and extension of the knee. It can also occur in a sub-acute form, with repetitive trauma, originating a process of tendinosis.
Acute ruptures course with sudden pain and a “snap” or “whiplash” sensation. The haematoma is extremely exuberant and may be visible over a large area of the buttock, thigh or leg. In cases of complete rupture, flexion of the knee is difficult, even against low resistance. In chronic tendinopathies progressive pain on active knee flexion or during stretching is frequent. Discomfort may occur at rest in the sitting position for prolonged periods. If there is compression and inflammation of the sciatic nerve, neurological complaints may dominate the clinical picture with pain radiating to the foot, numbness/tingling or loss of strength.
In the acute phase, conservative treatment with analgesia, ice and rest is the most recommended. Progressive physiotherapy and progressive muscle strengthening may be used.
In cases of rupture with persistent complaints despite conservative treatment, surgical treatment with fixation and anchoring of the joint tendon may be indicated. This may be done by mini-invasion or arthroscopically in recent ruptures, or by open surgery in cases with significant retraction of the tendons. Whenever there is a possibility of scar adhesions to the sciatic nerve, it should be carefully released in order to avoid persistent neurological complaints.